

It all starts with a detailed clinical analysis
Placing dental veneers can produce a result that is tailored to the patient’s age. In this article, we explain in detail this patient’s case.
This patient initially came to us looking to restore her oral health. Although aesthetics is currently an essential factor, the aim of any treatment should be to restore health, function and aesthetics in a sensible and conservative manner. The different areas of dentistry need to work together to solve the issues involved in each case. A multidisciplinary approach is therefore essential in order to realise a diagnosis and an appropriate treatment plan, in order to achieve satisfactory results.
After a detailed oral clinical analysis of this case, we identified numerous situations/problems that needed to be corrected and treated in order to achieve the desired functional and aesthetic results. That said, it was necessary to correct:
– Anterior deep bite / pronounced overbite: a normal anterior bite is considered when the upper front teeth overlap the lower teeth by 2 to 3mm. A larger than normal gap in the anterior and/or posterior region is called a deep bite and can be caused by a number of aetiologies, one of which is anterior and posterior tooth extrusion. This deep bite was causing generalised wear and fractures, which made the anterior rehabilitation of these teeth practically impossible due to the risk of fracture.
– Posterior deep bite/Posterior inverted smile: the fact that this patient had lost some lower posterior teeth without rehabilitating them promptly led to the extrusion of one or more teeth in the upper arch. This extrusion, in addition to compromising the space for lower rehabilitation, can cause joint and periodontal problems.

In this way, it would be necessary to promote the intrusion of the extruded posterior and anterior teeth. The intrusion of posterior teeth, compared to the instrusion of anterior teeth, is a more difficult movement to achieve due to the greater volume of the roots of molars and premolars, which leads to a longer treatment time if techniques other than conventional orthodontic appliances are not implemented. Before the appearance of micro-implants, the main alternatives for rehabilitating a patient with a group of extracted teeth in the posterior region were, in most cases, aggressive wear of these teeth or even their extraction. Today, with the aid of skeletal anchorage (the use of micro-implants), with or without the use of orthodontic appliances ( transparent brackets or aligners), it is possible to carry out dental intrusion.
Thus, after a detailed explanation and analysis of all the situations that would need to be corrected prior to oral rehabilitation, a final upper rehabilitation was proposed with 13 ceramic pieces (veneers, crowns and crowns on implants) and lower restorations, new crowns on implants and incisal edge augmentation restorations in composite. It should be highlighted that this final rehabilitation could now be carried out without any major risk of fractures, since health and function had been fully restored.

Treatment phases and execution time:
1- Assessment/Diagnosis appointment: Clinical examination, auxiliary diagnostic tests including orthopantomography (general radiographic examination) and CT (computerised tomography) and photographic protocol, in order to reach a correct diagnosis and define the appropriate treatment plan for the patient.
2 – Oral Hygiene appointment
3 – Primary Health Treatments: Before any rehabilitation treatment, it is essential to re-establish oral health (without any inflammatory or infectious process). Firstly, teeth 16 and 17 (upper molars) were extracted due to root fractures and extensive caries lesions, respectively. Subsequently, all the old composite restorations, which were infiltrated, maladapted and overflowing (teeth 24, 25, 26, 14, 44 and 34) were replaced. Lastly, tooth 15 (2nd premolar) had a periapical lesion in addition to an old unadapted crown. A new devitalisation and a new spike with a temporary PMMA (polymethacrylate) crown were carried out.
4 – Surgical phase: 3 months after the extraction of teeth 16 and 17, we placed 2 implants to replacing these teeth.
5 – Cementation of conventional upper and lower fixed appliances and placement of 2 micro implants: Initially, a conventional upper and lower fixed appliance (Brackets) was cemented to align and level the dental arches. However, due to the existence of an accentuated anterior and posterior deep bite, it was necessary to resort to the use of Micro-Implants since the desired intrusion was still considerable and the aim was to be as quick as possible in the treatment.
6 – Removal of micro-implants and fixed appliances, forwarding to Oral Rehabilitation;
7- Scan for crown replacement on posterior-inferior implants + anterior-inferior wax-up: Firstly, it was important to establish an ideal occlusion, one that allows all the functions of the Stomatognathic System to be carried out and preserves the constituent structures (2). As this is a case in which the vertical dimension of occlusion (VOD) has been lost, there is an occlusal imbalance. Re-establishing the maxillo-mandibular relationship is fundamental for an adequate oral rehabilitation to be carried out, thus restoring the lost aesthetics and function (3). Once the correct position of the lower jaw had been determined, it was then ascertained what the exact ideal OVD measurement was for the patient, idealising this study for a final lower rehabilitation with posterior composite restorations and replacement of the old crowns on implants, already with the correct increase in OVD.
7.1 Placement of posterior crowns + Lower anterior incisal edge restorations: After providing lower posterior support with the new crowns and composite OVD augmentation restorations, the lower incisal edge augmentation restorations were made, re-establishing the function and harmony of the smile.
7.2 Digital Planning/Engineering: After finalising the orthodontic treatment and increasing the OVD (vertical dimension of occlusion) at the expense of the lower arch, we proceeded with the digital design of the future upper smile, with ideal anatomy and aesthetics for the patient, based on the photographic record and intraoral scan taken.
7.3 Mock-up: This is a simulation of the patient’s idealised smile (test smile mock-up). The patient can see the individualised digital planning proposed for the final treatment plan “in their mouth” and “live”. It is an extremely useful communication tool for the patient and the dentist for the following reasons:
- Simulates the final result;
- The result is temporary and can be modified according to the patient’s preferences;
- It can be repeated as many times as necessary to achieve the best possible solution;
- Helps build trust between the patient and the dentist.
- Appointment for Dental Preparation and Impressions
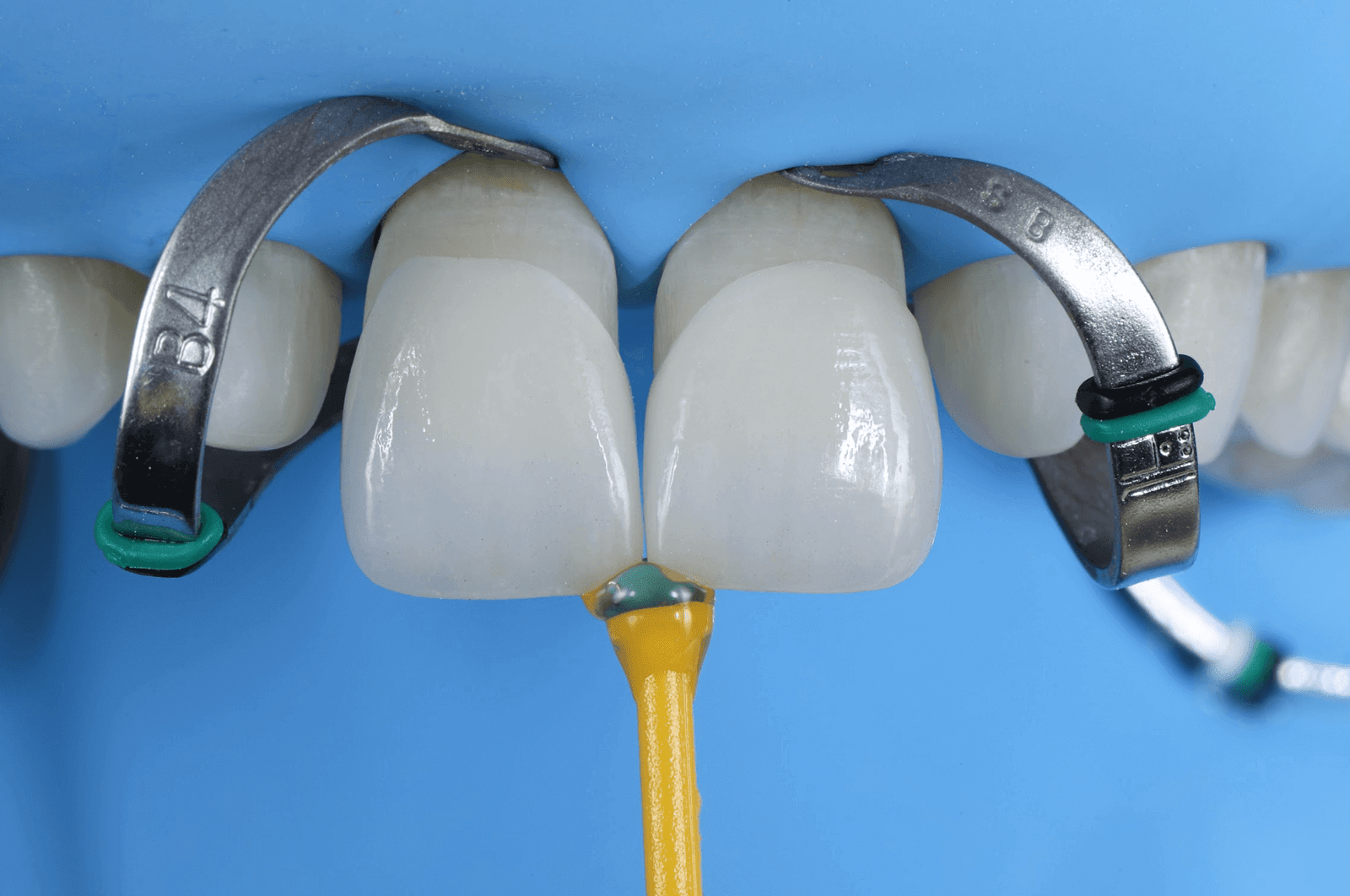
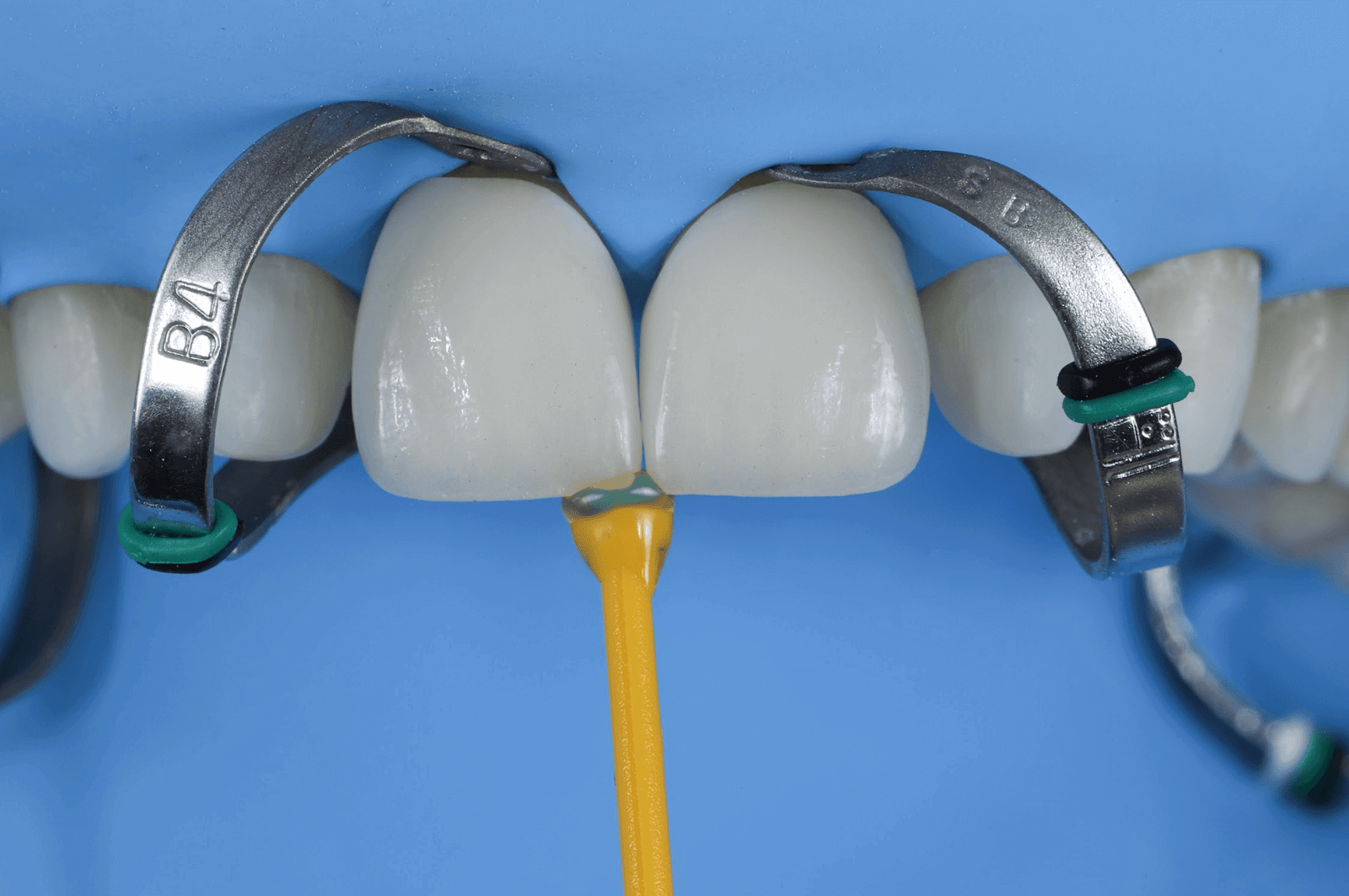
A well-planned and minimally invasive dental preparation directly influences the longevity of the treatment, as it provides better conditions for making the impression, better adaptation and fitting of the fabricated pieces, and most importantly, it provides the correct distribution of masticatory and occlusal forces in the restoration (4). Therefore, all the wear in this case was performed using wear wrenches, in the least invasive way possible, maintaining as much healthy tooth structure and enamel as possible. After the dental wearing, the digital and/or conventional impressions were carried out, which is essential for the laboratory technician to execute the work. Next, the provisional piece was placed, the aesthetics of which are similar to those presented to the patient in the mock-up. At this stage, the teeth are joined together and some precautions need to be taken when eating, such as avoiding foods that are too hard, crunchy or that cause pigmentation (beetroot, red wine, curry, etc.).
- Appointment for Adhesion/Cementation of the definitive work
After an average of one week, the provisional work is replaced by the definitive ceramic work. The entire bonding/cementation protocol was properly followed, respecting all the individual rules for each material.

- Occlusion Appointment
The importance of control and protection in oral rehabilitation begins with a multidisciplinary diagnosis and continues with the placement and control of a night stabilisation drip. It should be emphasised that in order to carry out an aesthetic rehabilitation, it is essential that it is functional and long-lasting. It is important to diagnose bruxism or other parafunctional habits.

The sharing of the images and the text referenced to them has been expressly authorised by the patient for this purpose.
The patient has specifically consented to and approved the publication of her health data and personal case to the exact extent that it is made public, as the information is truthful and objective, and could contribute to the free and informed choice of other patients.




